常见问题(不定期更新)
mango支持远端用户连接(创建用户)
> use target_db |
> use target_db |
| 名称 | 作者 | 打分 | 状态 | 类型 |
|---|---|---|---|---|
| 别闹了,费曼先生 | 费曼 | Reading | 传记 | |
| 量子和粒子物理学何以解释一切 | ⭐️⭐️⭐️⭐️ | Reading | 科普 | |
| 微积分的力量 | ⭐️⭐️⭐️⭐️⭐️ | Reading | 科普 | |
| 货币战争 | James Rickards | ⭐️⭐️⭐️ | Finished | 科普 |
| 费曼讲物理:相对论 | 费曼 | ⭐️⭐️⭐️ | Finished | 科普 |
| 丰乳肥臀 | 莫言 | ⭐️⭐️⭐️⭐️⭐️ | Finished | 小说 |
| 时间秩序 | Finished | 科普 | ||
| 白鹿原 | 陈忠实 | ⭐️⭐️⭐️⭐️⭐️ | Finished | 小说 |
| 南京大屠杀 | ⭐️⭐️⭐️⭐️⭐️ | Finished | 历史 | |
| 谷歌方法 | ⭐️⭐️⭐️ | Finished | 传记 | |
| 明朝那些事 | ⭐️⭐️⭐️⭐️⭐️ | Finished | 历史 | |
| 房思琪的初恋乐园 | ⭐️⭐️⭐️ | Finished | 小说 | |
| 邓小平传 | ⭐️⭐️⭐️⭐️ | Finished | 传记 | |
| 三体 | 刘慈欣 | ⭐️⭐️⭐️⭐️⭐️ | Finished | 小说 |
| 美国陷阱 | [法] 弗雷德里克·皮耶鲁齐 / [法] 马修·阿伦 | ⭐️⭐️⭐️⭐️ | Finished | 政治 |
| 球状闪电 | 刘慈欣 | ⭐️⭐️⭐️⭐️ | Finished | 小说 |
| 顺势而为:雷军传 | ⭐️⭐️⭐️ | Finished | 传记 | |
| 从一到无穷大 | ⭐️⭐️⭐️⭐️ | Finished | 科普 | |
| 万历十五年 | 黄仁宇 | ⭐️⭐️⭐️ | Finished | 历史 |
| 曾国藩传 | 张宏杰 | ⭐️⭐️⭐️⭐️ | Finished | 传记 |
| 显微镜下的大明 | 马伯庸 | ⭐️⭐️⭐️⭐️ | Finished | 历史 |
| Mysterious child hepatitis continues to vex researchers | ||||
| After Roe v. Wade: US researchers warn of what’s to come | Finished | |||
| How common is long COVID? Why studies give different answers | Finished | |||
| Nature Index Annual Tables 2022: China’s research spending pays off | Finished | |||
| How months-long COVID infections could seed dangerous new variants | Reading | |||
| Learn from COVID: Gates’s pandemic prescription | ||||
| COVID and smell loss: answers begin to emerge | Ready to Start | |||
| Opinion: Destroy All Samples of the Smallpox Virus | Finished | |||
| COVID death tolls: scientists acknowledge errors in WHO estimates | Finished | |||
| NASA’s Perseverance rover begins key search for life on Mars | Reading | |||
| The number of researchers with dual US–China affiliations is falling | Finished | |||
| ‘Unsustainable’: how satellite swarms pose a rising threat to astronomy | Finished | |||
| Epigenome Editing Decreases Alcohol Seeking and Anxiety in Rats | Finished | |||
| HHMI to Award More than $1 Billion to Promote Equity in Research | ⭐️ | Finished | ||
| Salmonella Injection Helps the Mouse Immune System Kill Tumors | Finished | |||
| Eight Weeks of Meditation Doesn’t Change the Brain, Study Finds | ⭐️⭐️⭐️ | Finished | ||
| Making the most of media interviews | ⭐️⭐️⭐️ | Finished | ||
| What’s the Evidence for Fluvoxamine in COVID-19? | ⭐️⭐️⭐️⭐️ | Finished | ||
| What to Know About the Defamation Trial Between Johnny Depp and Amber Heard As It Resumes | ⭐️ | Finished | ||
| LOVE-DEATH-ROBOTS | Finished | |||
| One Million Americans Have Died From COVID-19. Here Are Some of Their Stories | ⭐️ | Finished | ||
| US Case Adds to Unusual Monkeypox Outbreak | ⭐️⭐️ | Finished | ||
| More than 3,000 potentially harmful chemicals found in food packaging | ⭐️ | Finished | ||
| Link between COVID-19 and Parkinson’s disease risk grows with new findings | ⭐️ | Finished |
# git status 乱码 |
go env -w GOPROXY=https://mirrors.aliyun.com/goproxy/,direct |
cmd + shift + p 打开命令基本过程可描述为:每次寻找f(n)最小的点探索。
核心为: f(n) = g(n) + h(n)
其中: - f(n): 表示从起点到任意顶点n的分值、权重 -
g(n): 表示从起点到任意顶点n的实际距离 - h(n):
表示任意顶点n到目标顶点的估算距离(根据所采用的评估函数的不同而变化)
这个公式遵循以下特性: - 如果g(n)为0:
即不计算起点到n点的实际距离,只考虑n到终点的预估距离,算法变为贪心算法,快,但是不一定能找到结果
- 如果h(n)为0:
即不计算n到终点的估算距离,转化为Dijkstra算法
vsc启动时terminal报错,提示访问链接: https://code.visualstudio.com/docs/supporting/faq#_resolving-shell-environment-fails
按照提示,注释掉~/.bashrc or
~/.zshrc底下需要长时间操作的操作,例如nvm
重启vsc后正常。
去 官网 下载最新版本, 并安装

1.3.1 拉取工程 https://github.com/powerline/fonts
git clone git@github.com:powerline/fonts.git
1.3.2 安装字体
执行./install.sh指令安装所有Powerline字体 安装完成后提示所有字体均已下载到/Users/superdanny/Library/Fonts路径下
1.3.3 修改iterm设置

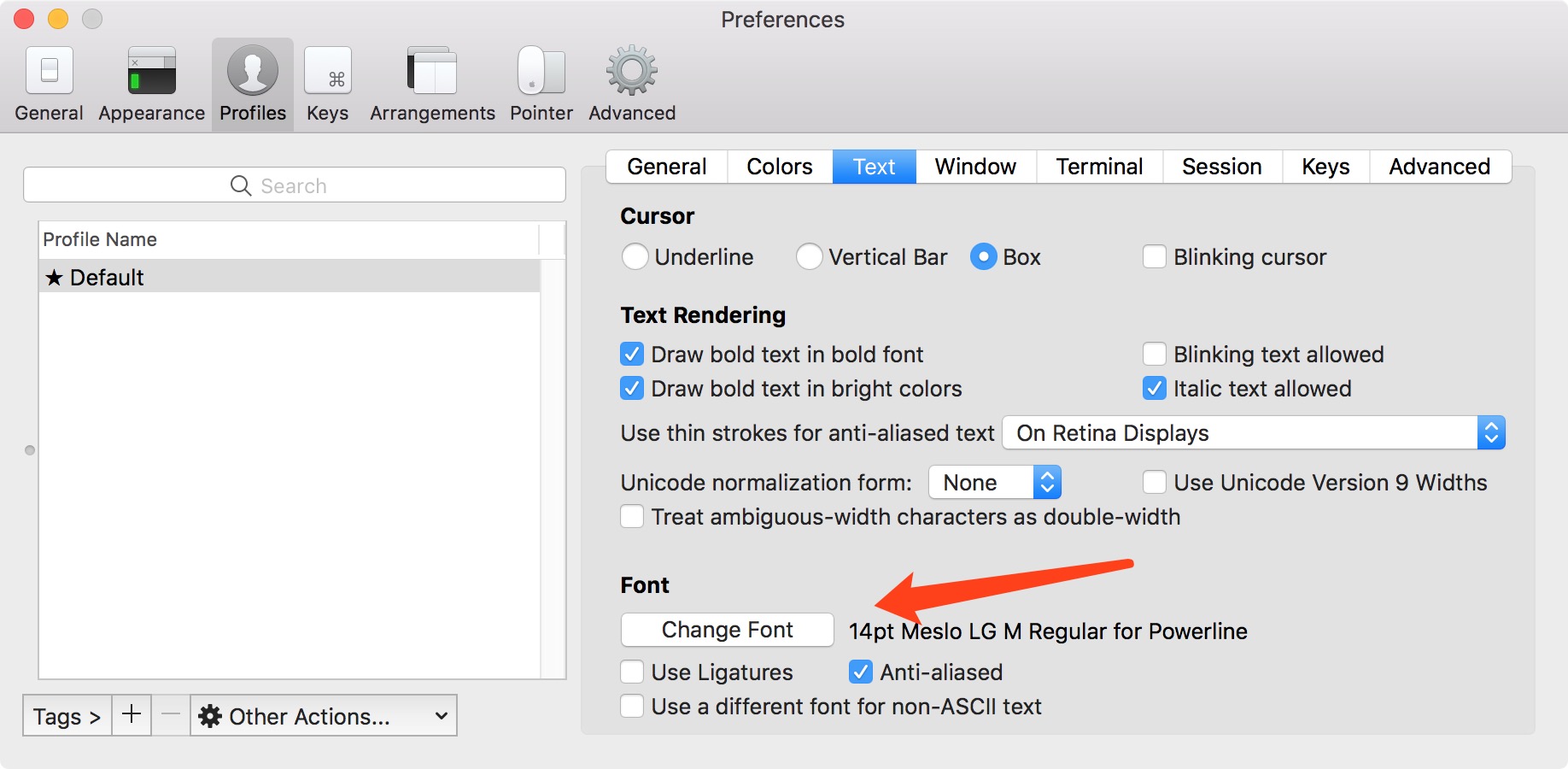
1.3.4 修改vsc terminal字体
配置中搜索 terminal font 或者
settings.json中"terminal.integrated.fontFamily"配置为Meslo
LG L DZ for Powerline
配置配色方案

via curl
sh -c "$(curl -fsSL https://raw.github.com/robbyrussell/oh-my-zsh/master/tools/install.sh)"
via wget
sh -c "$(wget https://raw.github.com/robbyrussell/oh-my-zsh/master/tools/install.sh -O -)"
通过 cat /etc/shells 命令可以查看当前系统可以使用哪些shell
通过 echo $SHELL 命令可以查看我们当前正在使用的shell
如果当前的shell不是zsh,我们可以通过 chsh -s /bin/zsh 命令可以将shell切换为shell之zsh,终端重启之后即可生效。
下载agnoster主题
到下载的工程里面运行install文件,主题将安装到~/.oh-my-zsh/themes目录下
设置该主题
进入~/.zshrc打开.zshrc文件,然后将ZSH_THEME后面的字段改为agnoster。ZSH_THEME="agnoster"(agnoster即为要设置的主题)
cd到.zshrc所在目录
执行指令将工程克隆到当前目录 git clone git://github.com/zsh-users/zsh-syntax-highlighting.git
打开.zshrc文件,在最后添加下面内容
plugins=(git zsh-syntax-highlighting)
保存文件。
使用homebrew安装
brew install pyenv |
.zshrc配置添加环境变量和脚本初始化环境
export PYENV_ROOT="$HOME/.pyenv" |
安装python和虚拟环境 pyenv install 3.10.4
# pyenv virtualenv <python version> <virtual name>
pyenv virtualenv 3.10.4 jx
配置完成之后,可以在路径下添加文件 .python-version
这样进入路径后会自动加载虚拟环境# .python-version
jx

| 单词 | 音标 | 释义 |
|---|---|---|
| epidemoic | [ˌepɪˈdemɪk] | 流行病 |
| annex | [əˈneks] | 附件 |
| Viet Nam | [viˈɛt næm] | 越南 |
| cumulative | [ˈkjuːmjələtɪv] | 累计的 |
| hazad | 危险、危害 |
Globally, during the week of 4 through 10 April 2022, the number of new COVID-19 cases and deaths has continued to decline for a third consecutive week, with over 7 million cases and over 22 000 deaths reported, a decrease of 24% and 18% respectively, as compared to the previous week (Figure 1).
总的来说,从4月4日~10日的这一周内,新的COVID-19确诊和死亡数已经持续下降了3个星期,共报道了超过700万的病例和22000例死亡,相比于上个星期分别下降了24%和18%
All regions reported decreasing trends in the number of new weekly cases and deaths (Table 1). As of 10 April 2022, over 496 million confirmed cases and over 6 million deaths have been reported globally.
所有区域最近一个星期从上报的数量来说都呈现下降的趋势。截止2022年4月10日,全球共报道超过496万确诊以及超过600万的死亡。
These trends should be interpreted with caution as several countries are progressively changing their COVID-19 testing strategies, resulting in lower overall numbers of tests performed and consequently lower numbers of cases detected.
这个趋势可以谨慎的解释为一些国家正在改变他们的检测策略,导致更低的检测数字,从而导致更低的确诊量
At the country level, the highest numbers of new weekly cases were reported from the Republic of Korea (1 459 454 new cases; -29%), Germany (1 019 649 new cases; -26%), France (927 073 new cases; -3%), Viet Nam (453 647 new cases; -43%), and Italy (447 322 new cases; -8%)
国家的等级上,最新的周确诊量最多的是韩国,德国,法国,越南和意大利
The highest numbers of new weekly deaths were reported from the United States of America (3 682 new deaths; -9%), Republic of Korea (2 186 new deaths; -6%), the Russian Federation (2 008 new deaths; -15%), Germany (1 686 new deaths; +6%), and Brazil (1 120 new deaths; -22%).
死亡数最多的是美国,韩国,俄罗斯联邦,德国,巴西。
WHO, in collaboration with national authorities, institutions and researchers, routinely assesses if variants of SARSCoV-2 alter transmission or disease characteristics, or impact effectiveness of vaccines, therapeutics, diagnostics or public health and social measures (PHSM) applied to control disease spread. Potential variants of concern (VOCs), variants of interest (VOIs) or variants under monitoring (VUMs) are regularly assessed based on the risk posed to global public health.
WHO,和国家当局、机构、研究者们合作,日常评估是否病毒变种改变传播途径或者病理特性,或影响疫苗、治疗、诊断或者公共卫生以及社会措施控制疾病传播的效用。根据公布的全球公共健康定期评估潜在的病毒变种,感兴趣的变种和监控中的变种。
The classifications of variants will be revised to reflect the continuous evolution of circulating variants and their changing epidemiology. Criteria for variant classification, and the current lists of VOCs, VOIs and VUMs, are available on the WHO Tracking SARS-CoV-2 variants website. National authorities may choose to designate other variants and are encouraged to investigate and report on the impacts of these variants. When referring to the genomic sequence of SARS-CoV-2 identified from the first cases (December 2019), the term ‘index virus’ should be used.
变种得分类将会修改,以反应流行变种得持续进化以及他们流行病学的变化。变种分类的标准,当前关注变种,感兴趣的变种,监控中的变种的列表,都可以在WHO变种网站上跟踪查看。国家当局可能选择命名其他变种,他们被鼓励调查和报道其他变种的影响。当参考第一例认证的基因序列时,需要使用“病毒索引”一词
The Omicron variant remains the dominant variant circulating globally, accounting for nearly all sequences recently reported to GISAID. Among the 379 278 sequences uploaded to GISAID with specimens collected in the last 30 days , 376 082 (99.2%) were Omicron, 125 (<0.1%) were Delta and 2 961 (0.8%) sequences were not assigned to a Pango lineage. These trends should be interpreted with due consideration of the limitations of surveillance systems, including differences in sequencing capacity and sampling strategies between countries, as well as laboratory turnaround times for sequencing and delays in reporting.
Omicron依旧是世界范围传播的主要变种,在过去的30填收集的379278份序列样本中,几乎所有序列都是Omicron ,其中376082份是Omicron ,125份是Delta,另外2961份未分具体类系。这个趋势可以解释为监测系统的局限性,包括国家之间测序的能力,采样策略的区别等,以及实验室测序和报告延迟的周转时间。
WHO continues to monitor several descendent lineages under the Omicron VOC, including BA.1, BA.2, BA.3 as well as now BA.4 and BA.5 . It also includes BA.1/BA.2 circulating recombinant forms, such as XE. The full list can be found here https://cov-lineages.org/lineage_list.html
WHO持续监控几个OMicron世系下的后代,包括。。。。。也包括循环重组格式的。。。。。所有的列表能在这里找到。
A small number of sequences of BA.4 and BA.5 descendent lineages have now been detected in a few countries. Both have additional mutations in the Spike region (S:L452R, S:F486V) and unique mutations outside of Spike. The S:L452R and S:F486V mutations are associated with potential immune escape characteristics. In addition, the majority of BA.4 and BA.5 sequences have the 69-70 deletion responsible for S gene target failure (SGTF) in some PCR assays. This may prove useful for surveillance purposes in places where BA.2 is dominant, as the 69-70 deletion is largely not present in BA.2 sequences.
某个分支的后代的序列在几个国家被检测到。都含有额外的突触突变和特别的外部突触。这些突变与潜在的免疫力逃逸特征有关联。
这应该可以证明有助于监测这几处。
WHO is working with scientists to further assess the characteristics of these lineages and their public health implications. WHO recommends countries to continue surveillance, where possible, and rapid data sharing on publicly available databases.
WHO整与科学家们合作评估这些世系的特性以及他们对于公共健康的影响。WHO建议各个国家持续监测,如果可能的话,快速分享数据。
The COVID-19 pandemic continues to evolve, as does our understanding of the SARS-CoV-2 virus, and the response needed to control its spread and impact. In WHO’s most recent rapid risk assessment, which was completed on 6 April 2021, the global public health risk was assessed to remain very high due to the ongoing risks to human health, risk of spread and risk of insufficient control capacities. Under the Emergency Response Framework, WHO undertakes risk assessments and situation analyses on a regular basis to inform its response to emerging situations. In addition, WHO periodically reviews the current risk status of public health events through an in-depth hazard, exposure and context assessment. This also includes a review of the vulnerabilities and capacities available to respond to the public health event and to investigate the current risk to human health, risks of ongoing spread globally, and risk of insufficient control capacities. Such assessments are used as an internal WHO decision-making tool, and to support independent deliberations, including but not limited to meetings of the International Health Regulations (IHR 2005) Emergency Committee regarding the COVID-19 pandemic.
To date, 13 global rapid risk assessments have been undertaken for COVID-19, and additional assessments have been conducted for specific events, such as the emergence of SARS-CoV-2 variants. Here, we provide a synopsis of the most recent in-depth global rapid risk assessment for COVID-19.
Despite a reduction in SARS-CoV-2 testing observed since the beginning of 2022 in many Member States, the COVID-19 pandemic continues with intense transmission and high levels of death primarily among unvaccinated at-risk populations. The highly transmissible Omicron variant of concern has rapidly replaced all other circulating variants in almost all countries in which it has been reported, and has become dominant globally.
Omicron’s properties of immune escape have been associated with the rapid and almost synchronous increase in the global incidence of COVID-19 cases reported until the end of January 2022. A further increase observed at the beginning of March was driven primarily by a delayed increase in case incidence in the Western Pacific Region and a rebound in the number of new cases reported in the European Region. This trend was likely due to a combination of factors, including the predominance of the Omicron Pango lineages BA.1, and then BA.2, with a transmission advantage over other Omicron lineages; relaxation of public health and social measures (PHSM); and waning of humoral immunity following vaccination and/or prior infection. The recent detection of emerging recombinants of the Delta-Omicron and Omicron descendent lineages requires ongoing close monitoring.
Unlike previous waves, the most recent wave due to Omicron can be characterized by a decoupling between the number of cases, hospitalizations (particularly for intensive care) and deaths in many countries. However, data continue to show that those who are unvaccinated remain at higher risk of severe disease following infection with Omicron as compared to those who have been vaccinated. Despite the reduction in severity, the massive increases 7 in cases with Omicron have led to large numbers of hospitalizations, putting further pressure on healthcare systems, and in some countries, similar or higher numbers of deaths when compared to previous peaks.
While vaccine effectiveness (VE) wanes against Omicron for all disease outcomes as compared to other VOCs following the primary vaccination series, VE estimates for Omicron remain the highest for severe disease. Furthermore, there is evidence that a booster dose substantially improves VE for all outcomes; however, more data are needed to characterize the duration of this protection.
Over 11 billion vaccine doses have been distributed globally. Nevertheless, substantial inequities remain, with only 11% of those in low-income countries (LICs) having completed the primary series; and major differences among regions, with vaccination coverage ranging from 82% in the Western Pacific Region to 13% in the African Region. There is particular concern about reaching the most vulnerable populations who remain unvaccinated, particularly those of older age and those with comorbidities. Globally, an estimated 35% of those aged 60 years and over are awaiting completion of the primary vaccination series. Despite low vaccination coverage in the African Region, the most recent estimates of combined seroprevalence (vaccine and infection-derived humoral immune response) were 72.6% (95% CI: 71.7-73.5%). Considering the low vaccine coverage, such seroprevalence estimates highlight the extent of SARS-CoV-2 transmission across the Region. WHO Emergency Use Listing (EUL) approved diagnostic tests, including nucleic acid amplification tests (e.g. polymerase chain reaction (PCR) assays) with more than one viral target or antigen-detection rapid diagnostic tests (Ag-RDTs), remain effective at detecting Omicron infection, including BA.1 and BA.2. WHO is concerned that during recent months, some countries have significantly reduced SARS-CoV-2 testing, despite widespread availability of diagnostic tests. Unless robust surveillance systems are retained, countries may lose the ability to accurately interpret epidemiological trends, implement the appropriate measures necessary to reduce transmission and monitor and assess the evolution of the virus.
Despite current high rates of transmission of SARS-CoV-2, many countries have dropped most PHSM without following a layered or staged approach to relaxation. This can lead to the erosion of public trust and PHSM may not be easily re-implemented should the future need arise, for example following the emergence of a new VOC. Each country faces different circumstances based on the epidemiological situation and the context. WHO has published an updated Strategic Preparedness, Readiness and Response Plan to End the Global COVID-19 Emergency in 2022 which outlines future scenarios of COVID-19 and how the current strategy needs to be adjusted taking into account the difficulties posed by the pandemic in the light of the many other public health and global challenges. This is particularly apparent during other emergencies including the war in Ukraine and protracted conflicts in many other countries.
The confidence in the available information on the global public health risk remains moderate. There are still gaps in knowledge about the phenotypic impact of emerging SARS-CoV-2 variants and recombinants; the long-term duration of infection and vaccine-derived protection, particularly against severe disease and hospitalization; and the impact of lifting and changing PHSM on transmission, hospitalization and mortality.
眼睛越来越不行了。为了保护眼睛。搜索了如何全页面深色模式
需要Google Chrome版本 高于78。